News & Publications
Distinguishing Adenocarcinoma from Squamous Cell Carcinoma of the Lung
November 10, 2013
By David C. Hoak, M.D.
Prior to a patient beginning lung cancer treatment, it is important for an experienced lung cancer pathologist to review each case. This is a critical step because small cell lung cancer responds well to chemotherapy, is generally not treated surgically, and can be confused with non-small cell carcinoma on initial microscopic examination. In addition, the response to certain drug regimens in patients with non-small cell carcinoma (NSCLC) with adenocarcinoma is different from squamous cell carcinoma patient response.
The response to certain drug regimens in patients with non-small cell carcinoma (NSCLC) with adenocarcinoma is different from squamous cell carcinoma

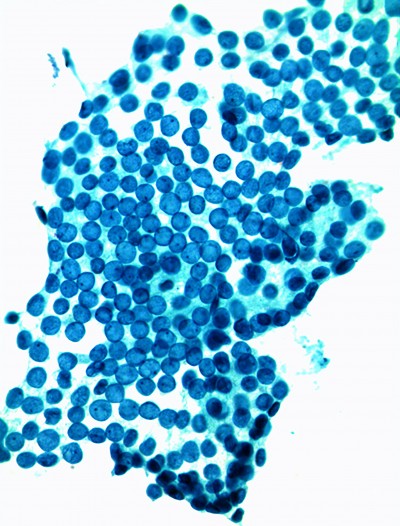
Napsin A staining reveals adenocarcinoma of the lung
At the time of biopsy, the pathologist and especially the cytopathologist play a pivotal role in the appropriate triage of these often tiny specimens. The significant clinical implications of determining adenocarcinoma from squamous cell carcinoma include:In an article in the May 2011 issue of CAP Today titled, “Use of Cytology and Small Biopsy Specimens in Diagnosing and Treating Lung Cancer,” the importance of distinguishing adenocarcinoma from squamous cell carcinoma early on is discussed. In addition, the article states it was previously believed that only histologic material was appropriate for sub-typing of non-small cell carcinoma. However, today’s IHC stains work well in small biopsy and cytology material, allowing the separation of adenocarcinoma from squamous cell carcinoma with an accuracy of up to 100 percent.
- Selection of the most effective drug regimen
- Avoidance of a potentially harmful drug regimen
- Triage of NSCLC for molecular mutation analysis.
At Incyte Diagnostics, we have our own panel of immunohistochemical markers for NSCLC which includes TTF-1, napsin A, CK5, CK7 and p63. TTF-1 and napsin A are the most commonly used stains to support glandular differentiation, which is important to determine a diagnosis of adenocarcinoma. TTF-1 (thyroid transcription factor-1) is known as a thyroid specific enhancer binding protein and is used to determine if a tumor arises from the lung or thyroid.
A positive TTF-1 stain supports a diagnosis of adenocarcinoma originating from the lung. The use of p63 stain is the preferred choice to support squamous differentiation. There can be some overlap in the staining between adenocarcinoma and squamous cell carcinoma, however it is exceedingly rare for squamous cell carcinomas to lack p63 expression. Any amount of p63 positivity along with a negative TTF-1 stain would indicate squamous differentiation.
| Adenocarcinoma | Squamous Cell Carcinoma |
| CK5 - | CK5 + |
| p63 - | p63 + |
| TTF + | TTF - |
| CK7 + | CK7 - |
| napsin A + | napsin A - |
If a tumor stains positive for both TTF-1 and p63, it is more likely to be an adenocarcinoma than a squamous cell carcinoma because TTF-1 is a more sensitive marker than p63. Cytokeratin (CK) 5 positivity can be seen in undifferentiated large cell carcinoma as well as squamous carcinoma of the lung. CK 7 is valuable to determine some adenocarcinomas. These stains also work well in cytology cell blocks which can be valuable when there is a limited amount of material to test. Correct application of TTF-1 and p63 can avoid misclassification of the tumor.
Lung cancer remains the leading cause of cancer-related mortality in the United States with and 157, 300 deaths and 222,520 new cases diagnosed in 2010 alone. Its diagnosis is challenging for all pathologists, and has become more so as additional special testing is requested on even smaller samples in the diagnosis of non-small carcinoma of the lung. Careful pathologic handling of all tumor material, whether it is surgically resected or minimally obtained, may result in earlier clarification of tumor type. This will lead eventually to better patient care management and eventually improved morbidity rates.